


A Hug for the Diagnosed
Mental suffering is real, "disorders" can be fictional


(This issue of The Mind Hug is inspired by Dr. David Burns’ thoughts on the DSM’s utility)
According to the Bible of Mental Disorders (the DSM-5, which defines “disorders”), for Major Depressive Disorder to be diagnosed, certain symptoms must exist most of the day for 14 days. ‘Most of the day’ - such impeccable precision. And it has to be 14 days. Essentially creating an illness at that arbitrary cut-off point, where none existed before. Poof - from a healthy to a disordered brain in a minute.
I admit that I am being a bit facetious here - it is only so that I can do some justice to illustrating the almost comical reality of how the DSM-5 looks at complex human suffering, and creates neat little boxes of “illnesses”. In the process, it invents simplistic labels, smooths over the rough edges of disparate individual distress, and creates an environment where diagnoses-driven manualised protocols (which treat the labels, and not the person) become extremely attractive. It also possibly gives the false impression that we know a lot more about the brain-mind connection than we actually do.
Quick Essential Note: There are exceptions of course, where the DSM-5 is helpfully conceptualising problems that have very specific brain anomalies and/or psychological symptoms (e.g. schizophrenia, OCD, and more). The intent of this article however, is to highlight how the DSM-5 takes too much unwarranted liberty in creating definitions around symptoms - definitions which tend to be accepted as specific truths about “things” that exist, like diabetes or cancer. The reality of the unique psychological pain of the individuals is not well served with such oversimplifications.
Comfort in Labels?
In the midst of utter confusion, suffering, and an amorphous psychological opponent, individuals seeking help often find comfort in labels and diagnoses. It is very understandable, I myself found comfort in my particular diagnosis: suddenly, that hazy cloud of vast distress, had a name, and therefore, engendered hope. As I later found out, however, my individual experience was too unique to benefit a great deal from a label.
Doctors, psychiatrists, and therapists (and all other humans) find comfort in labels - our brains are evolutionarily wired to seek patterns and label things so that we can navigate through a complex world. It is a nice cozy feeling to know. And then, there is the slippery slope from knowing to curing, using protocols (the pill for an ill model), without doing the extra work of individualising treatment.
Knowing, therefore, can at times create a dangerous finality of judgement.
All therapists, no matter how experienced, are prone to this error in my opinion - because our brains have also evolved to avoid tedious thinking and instead find shortcuts. Playing the “expert” is so tempting, with many rationalisations coming to our aid.
I believe both the medical professionals and the “diagnosed” can suffer a negative impact of taking diagnoses too seriously and not taking the actual pain seriously enough. Additionally, avoidable stigma associated with being “mentally ill” rears its ugly head for many individuals. If, like myself, the idea of a diagnosis, the stigma, the frustration with oversimplification, or any other aspect of this trigger-happy-disorder-defining approach rubs you the wrong way, the following are a few ideas to ponder over that have been helpful to me.

A Hug for Discomfort with Labels
The following ideas can help you take a non-pathologising, open and curious stance towards “disorders”:
Context: The DSM was originally a statistical tool, for research purposes. If two researchers were studying depression, they had to define some criteria as to what constituted a depressed person, so that they could agree on what they were studying. Lo and behold, arbitrary cut-off points were decided (14 days of symptoms, for example) and gradually this statistical definition assumed the shape of a “diagnosis” of a “disorder”. See the subtle but insidious issue here?
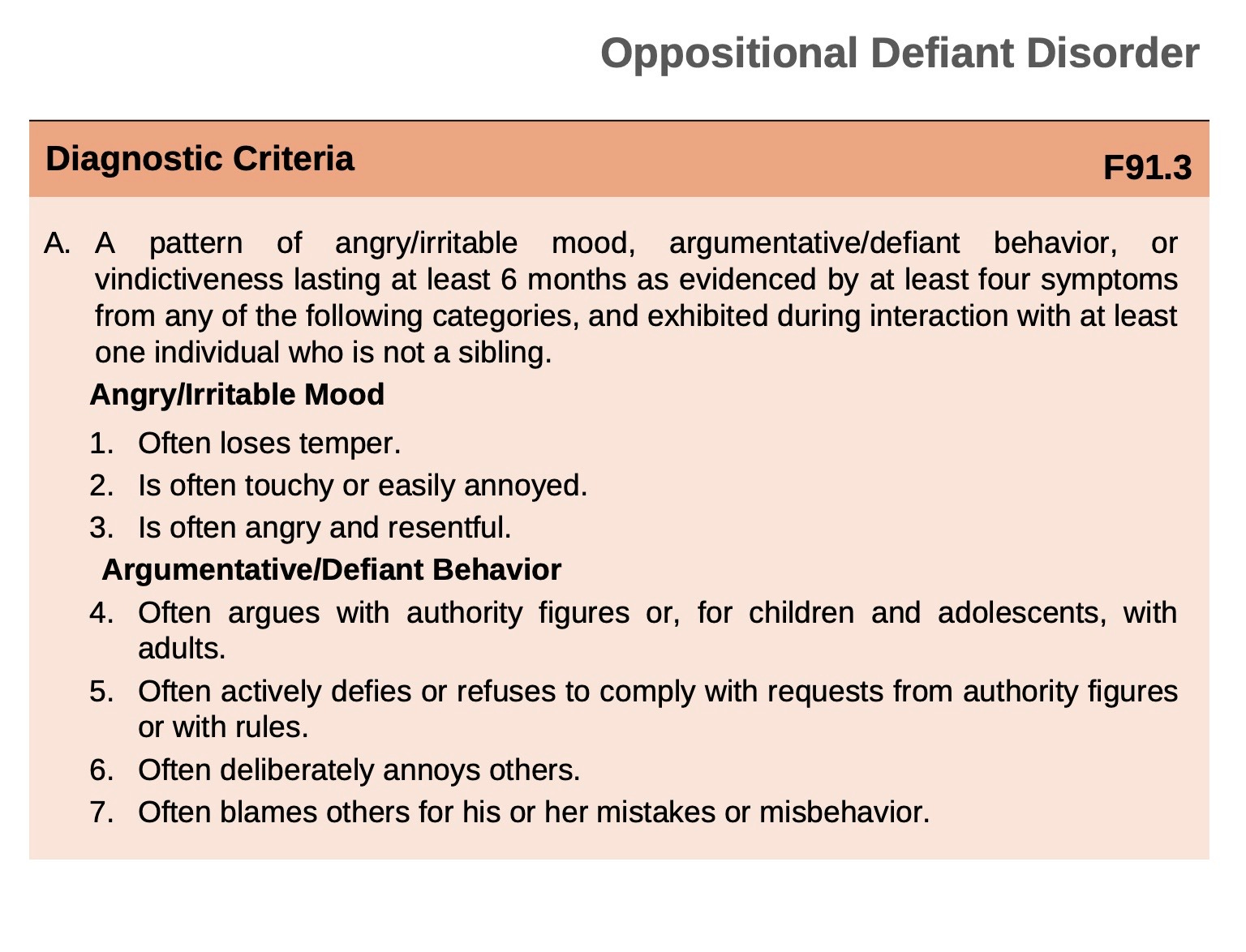
Universal Human Traits Pathologised: Look at the following diagnosis for instance: with “often”prepended to normal human tendencies and a 6 month arbitrary cut-off decreed, “Oppositional Defiant DISORDER” is born.

Usage of Vague Terms: The above diagnosis being a case in point: ‘touchy’, ‘deliberately annoys’, ‘blames’ etc. How touchy is disease-worthy touchy? Who doesn't deliberately annoy someone? How much annoyance would you reckon qualifies for a diagnosis? Would you also incorporate the subjective experience of the annoy-ee to really be precise? The usage of “often” itself, is quite an epitome of operationalised science. Who defines “often”? Dr. Dee S. Em: “This kid seems to annoy me a bit too often”.
Medical Model’s Shortcoming: In the domain of mental health, the medical model which is based on dichotomies (diseased vs. non-diseased people), falls short. Take shyness for instance. There is a huge variance in the amount of shyness and anxiety people experience in social situations (unlike fever for instance, where either you have a fever or you do not). If we were to draw a curve for shyness in the human population, it would be something of a bell curve. The DSM-5 essentially invents a false dichotomy by creating an arbitrary cut-off point for “too much shyness”, and calls it SOCIAL ANXIETY DISORDER! One can keep this reality-check in mind: normal human traits can get amplified, that does not necessarily mean a disorder exists.
In physiology, you wouldn’t say: “When the malignant tumour is in at least three organs and has often been causing the person pain, it is a diagnosis of the illness known as cancer”.
But the DSM gets away with it.
Your Symptoms May Differ from the Diagnosis: And that is alright. Now that you have a different vantage point on diagnoses, you can understand why online lists of symptoms might tell a different story. It can potentially frustrate and alienate diagnosed individuals who do not see their experience reflected in the “official list” of symptoms. Reminding ourselves of the massive short-comings of the DSM criteria, can help us make peace with the disparity.
Psychiatrist Visits: A psychiatrist who is well-informed pertaining to the statistical and arbitrary nature of the DSM-5, would hesitate in throwing around labels at you in a casual manner. She would educate you on what a particular diagnosis would mean, and would sprinkle a good dose of disclaimers on top of it. I would personally prefer such psychiatrists over the ones who can confidently say to me: “You have XYZ. You HAVE it. You caught it somewhere. Here is the pill for the ill, off you go to be healed”.
A Hug for Those Who Diagnose
“Psychiatry is conventionally defined as a medical speciality concerned with the diagnosis and treatment of mental diseases. I submit that this definition, which is still widely accepted, places psychiatry in the company of alchemy and astrology and commits it to the category of pseudoscience. The reason for this is that there is no such thing as “mental illness”.”
Thomas S. Szasz, The Myth of Mental Illness
I do not completely agree with Dr. Szasz, even though I resonate with the spirit of his message, especially because it is true most of the time.
But for those well-meaning, dedicated, and passionate doctors who have been initiated into the medical model of treating psychological suffering, I send a hug. In the echo chamber of that universe, it is increasingly difficult to see the fallacies within the fabric of the system. Add to it the money involved in medicating “consumers” (for an in-depth entertaining analysis, watch: Medicating Normal), it is easy to to see why the economic forces alone would resist any shock to the status quo.
Among those who are completely sold on this model, are professionals who have diligently studied psychiatry for the benefit of mankind, and it is my hunch that many of them would be disillusioned with it one day owing to an honest quest for truth they embody. After all, many of the greatest minds revered in the world of mental health, started off as doctors trained in the medical model (Aaron Beck, Thomas Szasz, Irvin Yalom, David Burns, to name a few).
I would love to hear from you. What has your experience been with psychiatry and diagnoses? If you are a psychiatrist or a therapist, what are your thoughts on the subject?
Until the next issue in November, I’d love to carry on a discussion here on Substack!